This article should be taken with a grain of salt (lacking all the information and details, sensationalist media slant to a controversial topic) but my intial reaction is that something unsavory occured. Basically, a transplant surgeon was a little too involved in expediting a donor's transition from "life" to "death". Now the whole concept of what constitutes "death" is actually a very complicated and controversial issue, especially in an age where advances in medical technology allows patients to be maintained on machines for years and years. In the old days, death was easy to define. The patient stopped breathing, the heart stopped and there wasn't anything you could do about it. You started calling funeral homes. Nowadays, however, "life" can be extended via artificial means. The distinction between life and death blurred as patients, formerly vibrant humans with personality, aspirations and desires, were reduced to existing organisms, maintained by machines and feedings that dripped through tubes into their stomach. The ethical implications of this distinction have become more prominent as transplantation has become the standard of care in dealing with such medical crises as chronic renal failure, liver failure, and heart disease. When is it ok to harvest viable organs from a patient? The infamous quote of "18 people die a day waiting for transplants" has put pressure on society to better define death and to come up with a better way for the equitable distribution of potentially life saving organs. There are two "official" definitions of potential organ donors: brain death and irreversible cardiac death.
In 1981, the President's Commission for the Sudy of Ethical Problems in Medicine and Biomedical and Behavioral Research defined "brain death" as follows:
-Unresponsiveness
The patient is completely unresponsive to external visual, auditory, and tactile stimuli and is incapable of communication in any manner.
-Absence of cerebral and brain stem function
Pupillary responses are absent, and eye movements cannot be elicited by the vestibulo-ocular reflex or by irrigating the ears with cold water.
The corneal and gag reflex are absent, and there is no facial or tongue movement.
The limbs are flaccid, and there is no movement, although primitive withdrawal movements in response to local painful stimuli, mediated at a spinal cord level, can occur.
-Apnea Test: An apnea test should be performed to ascertain that no respirations occur at a PCO2 level of at least 60 mmHg. The patient oxygenation should be maintained with giving 100% oxygen by a cannula inserted into endotracheal tube as the PCO2 rises. The inability to develop respiration is consistent with medullary failure.
-Nature of coma must be known
Known structural disease or irreversible systemic metabolic cause that can explain the clinical picture.
Some causes must be ruled out
Body temperature must be above 32 C to rule out hypothermia
No chance of drug intoxication or neuromuscular blockade
Patient is not in shock
-Persistence of brain dysfunction
Six hours with a confirmatory isoelectric EEG or electrocerebral silence, performed according to the technical standards of the American Electroencephalographic Society
Twelve hours without a confirmatory EEG
Twenty-four hours for anoxic brain injury without a confirmatory isoeletric EEG
-Confirmatory tests (are not necessary to diagnose brain death)
EEG with no physiologic brain activity
No cerebral circulation present on angiographic examination( is the principal legal sign in many European countries)
Brain stem-evoked responses with absent function in vital brain stem structures
Brain death is essentialy complete and irreversible cessation of all brain activity. This means that function has ceased in the cerebrum (the seat of consciousness) and also the more primitive, less complex parts of the brain such as the mid brain and brainstem. The patient cannot think, feel, or breath. This does not include people who are in a "persistent vegetative state", where higher cortical function has ceased, but spontaneous breathing and basic reflexes are preserved. After consultation with family members, the decision is made to donate the organs. The donor is wheeled to the OR while still on the ventilator. The heart contnues to beat. The harvest takes place while the organs are still being perfused by circulating blood, therefore making them more viable, less injured, and more easily preserved for use by a recipient. These are the ideal donors. The organs are alive right to the end. Immediately, once detached from the donor body, they are flushed with perfusate and put on ice. Shipped via helicopter to an eager recipient hours away.
Unfortunately, not enough people meet the criteria of brain death to satisfy the demand for organs. Severe head trauma or major strokes can render a person in a periststent vegetative state (PVS), without hope of recovery, without meaningful existence. So the other option is to define death by cessation of cardiac activity. Families who agree to this form of organ donation (non-heart beating donors) must understand that their loved one will be wheeled to the OR whereupon the ventilator will be disconnected and all life support withheld. What happens is, a bunch of medical personnel stand around looking at the monitor, waiting for the heart to go asystolic. When that occurs, the law requires a 5 minute waiting period, "just to make sure", and then the transplant team is allowed to commence the harvest. It sounds, and is, just a little ghoulish. Check out this link for a great selection of philosophic stances on the issues involved in the ethics of donation and transplantation.
My feeling is that it's all much ado about nothing. True, the 5 minute waiting period is arbitrary. But who cares. Why even wait five minutes? Each second of ischemia that passes makes those donor kidneys less likely to be a long term solution to another patient's renal failure. Why go through the charade of making sure various arbitrary criteria are met before proceeding with transplantation? Obviously, the process ought to be conducted in such a way that preserves the dignity of the donor, but not at the expense of wasting organs that could potentially save the life of another sentient, fully conscious human being. Patients in PVS do not have a meaningful existence. There's nothing anyone can say to dissuade me from that stance. Human life transcends mere "existence"; we are self aware beings who think, feel, and create. Simply oxygenating the billions of living cells in our body in not Human Life. It's beneath us.
What happened in California is unclear, but I can guess the basic scenario. The donor came to the OR and was disconnected from the machines but the heart kept beating. Maybe only 20 beats/minute or so, but it wouldn't stop. The official designation of "cardiac death" proved elusive. The transplant team got restless. Maybe they had flown in the middle of the night in a turbo prop plane to harvest the organs themselves. They didn't want to go back empty handed. So the Transplant surgeon enetered the OR and started to give meds; morphine, ativan. The betadine that was alluded to in the article was probably not given systemically (absurd) but maybe he prepped the abdomen and flushed some it through an indwelling feeding tube to make sure everything was sterile and ready to go for the harvest. Who knows. Certainly, given the current legal defintions, the surgeon's presence in the OR prior to the donor's official "death" seems a little unscrupulous. Hastening the demise of a donor, although reasonable from a utilitarian perspective and the perspective of potential recipients, is probably not the sort of activity America/society is ready to condone yet. The fact that the surgeon is up against criminal charges seems ludicrous to me. Did he break protocol and create the perception of a conflict of ineterst? Yes. Did he draw unnecessary, negative attention to a field that is already struggling to attract a big enough pool of donors and perpetuate the stereotype of transplant surgeons as predatory organ harvesters? Of course....
Hopefully something good can come out of it; in the form of a more open dialogue between physicians and patients about end of life issues. More honesty and putting more of the responsibility on the backs of family decision makers will, in the long run, lead us out of any legal quandaries. Why not present the case as such: "Ma'am, your husband is in a persistent vegetative state. You know this because he hasn't responded to you in the four years since the accident. We appreciate your intentions to donate his organs but you need to understand what will happen for this to occur. When the machine is turned off, his heart may stop quickly or it may not. If it slows but doesn't stop, the organs you wish to donate may be jeopardized. Do you wish for us to give medications that will hasten the complete cessation of his heartbeat, or do you wish that let nature take its course?"
Thursday, February 28, 2008
Perspective
It all depends on your point of view. I have this old guy who came in last week with a bowel obstruction from an incarcerated ventral hernia. He's 88, frail, and a walking medical disaster; CHF, 20% ejection fraction, chronic renal failure, severe COPD, and untreated lung cancer. Well I took him for OR and fixed the hernia and the bowel looked viable and he went to the ICU extubated. The next day, he was still breathing on his own and his hemodynamic parameters, although not great, were fairly decent. As far as I was concerned, he looked pretty damn good, given the circumstances, and I wrote as such in my progress note. When I stopped by later in the evening, I reviewed the chart to see what the other consultants were writing (surgeons like to read about how other doctors are impressed by their work). The pulmonologist actually wrote "looks awful". The hospitalist wrote "prognosis extremely grim". The nephrologist wasn't too impressed either. I was flabbergasted. Well, now he's post op day #6 and he's out of the ICU. Not so "awful" anymore......
Wednesday, February 27, 2008
Feeding Tubes
Few phone calls are more annoying for a general surgeon than the inevitably late night ER page about a patient from a nursing home who is "having problems" with a feeding tube that you may or may not have placed. It's clogged. It's leaking. It fell out. It hurts. And most medical personnel are terrified of them. No one knows exactly what to do and so it gets dumped on us.
Feeding tubes are an alternative to stuffing food down your mouth. Instead of filet mignon or smoked salmon, you get to infuse delicious Boost through a thin silastic or rubber tube directly into the stomach or small bowel, bypassing your taste buds and any enjoyment usually associated with eating. This isn't something you want. Unfortunately, certain conditions make them necessary such as strokes, swallowing difficulties, chronic aspiration, esophageal tumors, and other states of inanition. You also find feeding tubes placed in certain post-operative patients (Whipple, Gastric and esophageal tumors) as a way to provide enteral nutrition while more proximal anastomoses are healing.
Feeding tubes come in 2 varieties:
1. Gastrostomy tubes. These tubes are inserted into the stomach. More commonly nowadays, these tubes are placed percutaneously (Percutaneous Endoscopic Gastrostomy...PEG). Open or laparoscopic G-tubes are also an option if the percutaneous route is not available. G-tubes provide a little more flexibility in terms of feeding schedules because the stomach is such a large reservoir. Bolus feeds and continuous feeds are options. It's also easier to give medicines via a G-tubes because generally the tubes themselves are of largr caliber.
2. Jejunostomy tubes. These tubes are best used for feeding purposes when the stomach is not suitable or available. Now the jejunum is of a much narrower caliber than the stomach. Bolus feeds usually don't work and I worry about giving medicines, even crushed, via J-tubes because of clogging issues.
Biggest problems:
1. Clogged tubes. This is almost universally a result of poor nursing management. Enteral tube feed formulas are like wet cement; as long as the flow is steady and constant there's no worries. But if the feeds are turned off and the wet cement is allowed to stagnate in the tubing, it quickly solidifies and completely obstructs the lumen. The key is prevention and this means q4 hour flushings with saline or water. And any time the feeds are stopped (patient being transported somewhere) you HAVE TO FLUSH THE TUBE! It's an entirely avoidable complication as long as the tube is appropriately flushed on a regular basis. Most of the time I can clear it by power flushing the tube, but sometimes you have no choice but to replace the entire tube. Just thinking about this complication makes my heart rate accelerate because it's due to laziness.
2. Leaking tubes. Over time the exit site on the skin can sometimes enlarge and you can get minor enteric leakge on the abdominal wall. Lots of bile leakage should alert you to the possibility of distal bowel obstruction, or even a defect in the tubing itself.
3. Tubes that fall out. Happens all the time. Usually it's an elderly lady at the nursing home, demented and confused who yanks it out unknowingly. Most of time, especially with G-tubes, I can simply put another tube in through the established tract. Expediency is the key. The more time that elapses with the tube out, the harder it is to place a new one because scar tissue starts to form. J-tubes are a little dicier because I worry about perforating the bowel wall with blind insertion into the narrow jejunum; I like doing these with fluoroscopic guidance to confirm that the tip is actually within the lumen of bowel.
Feeding tubes are an alternative to stuffing food down your mouth. Instead of filet mignon or smoked salmon, you get to infuse delicious Boost through a thin silastic or rubber tube directly into the stomach or small bowel, bypassing your taste buds and any enjoyment usually associated with eating. This isn't something you want. Unfortunately, certain conditions make them necessary such as strokes, swallowing difficulties, chronic aspiration, esophageal tumors, and other states of inanition. You also find feeding tubes placed in certain post-operative patients (Whipple, Gastric and esophageal tumors) as a way to provide enteral nutrition while more proximal anastomoses are healing.
{kind=link}
Feeding tubes come in 2 varieties:
1. Gastrostomy tubes. These tubes are inserted into the stomach. More commonly nowadays, these tubes are placed percutaneously (Percutaneous Endoscopic Gastrostomy...PEG). Open or laparoscopic G-tubes are also an option if the percutaneous route is not available. G-tubes provide a little more flexibility in terms of feeding schedules because the stomach is such a large reservoir. Bolus feeds and continuous feeds are options. It's also easier to give medicines via a G-tubes because generally the tubes themselves are of largr caliber.
{kind=link}
2. Jejunostomy tubes. These tubes are best used for feeding purposes when the stomach is not suitable or available. Now the jejunum is of a much narrower caliber than the stomach. Bolus feeds usually don't work and I worry about giving medicines, even crushed, via J-tubes because of clogging issues.
{kind=link}
Biggest problems:
1. Clogged tubes. This is almost universally a result of poor nursing management. Enteral tube feed formulas are like wet cement; as long as the flow is steady and constant there's no worries. But if the feeds are turned off and the wet cement is allowed to stagnate in the tubing, it quickly solidifies and completely obstructs the lumen. The key is prevention and this means q4 hour flushings with saline or water. And any time the feeds are stopped (patient being transported somewhere) you HAVE TO FLUSH THE TUBE! It's an entirely avoidable complication as long as the tube is appropriately flushed on a regular basis. Most of the time I can clear it by power flushing the tube, but sometimes you have no choice but to replace the entire tube. Just thinking about this complication makes my heart rate accelerate because it's due to laziness.
2. Leaking tubes. Over time the exit site on the skin can sometimes enlarge and you can get minor enteric leakge on the abdominal wall. Lots of bile leakage should alert you to the possibility of distal bowel obstruction, or even a defect in the tubing itself.
3. Tubes that fall out. Happens all the time. Usually it's an elderly lady at the nursing home, demented and confused who yanks it out unknowingly. Most of time, especially with G-tubes, I can simply put another tube in through the established tract. Expediency is the key. The more time that elapses with the tube out, the harder it is to place a new one because scar tissue starts to form. J-tubes are a little dicier because I worry about perforating the bowel wall with blind insertion into the narrow jejunum; I like doing these with fluoroscopic guidance to confirm that the tip is actually within the lumen of bowel.
Tuesday, February 12, 2008
The Privilege
The other day I was re-consulted on a lady I knew from last month. She initially presented with weight loss, abdominal distention, and pain. The work-up showed a distal large bowel obstruction, a large pancreatic mass, and multiple liver metastases. The primary issue at the time was the colon obstruction; she was quite tender and was developing a leukocytosis. I explored her and found some sort of hard, fibrotic mass down in the pelvis. I couldn't differentiate rectum from gyne organs from bladder, so I simply gave her a loop sigmoid colostomy. Intra-operative biopsies of the pancreas and liver unfortunately revealed poorly differentiated adenocarcinoma. She was pretty much cooked. But at least she was diverted and could conceivably live out the rest of her days comfortably.
She returned a month later with abdominal distention and emesis. The CT scan this time suggested a high grade small bowel obstruction. We put in a NG tube and watched her. The she removed the NG and refused to have it put back. Her abdomen remained distended and she started to have pain. Every day, she looked a little worse, a little more beaten. Finally, the pain intensified, she was asking for morphine every half hour, and her WBC count crept up near 18k. Obviously, she needed an operation for definitive treatment but she'd been consistently refusing invasive procedures for the past several days. She had a terminal illness. Doing nothing was an understandable option. I spent a long time talking to the family, informing them and her of the options. You're in a bad way, I said. You're in no condition to tolerate another major abdominal operation, but dying from a bowel obstruction isn't pleasant either. I sat on the edge of her bed while her family crowded around, her husband in a chair holding her hand across from me. These moments in medicine are so raw and private and absolutely pure. As doctors, we are privileged to be able to participate in these intimate discussions of life and death. Almost like voyeurs, we walk into their lives when they are most vulnerable, when all pretense is washed away and the very essence of one's existence is at stake, and they welcome our presence, stranger that we are, because they need us there........She looked at her kids, then her husband. I can't do it anymore, she says. I just can't. I'm tired of it all. I want to rest. Can't you just give me something for the pain....
Her husband's head dropped and he squeezed her pale thin hand even tighter. Sure honey he said, his voicing barely holding together. We can do that. Right doctor? I nodded my head and rose slowly from the bed. Silently, I made my way out of the room; my privileged time had come to an end.
She returned a month later with abdominal distention and emesis. The CT scan this time suggested a high grade small bowel obstruction. We put in a NG tube and watched her. The she removed the NG and refused to have it put back. Her abdomen remained distended and she started to have pain. Every day, she looked a little worse, a little more beaten. Finally, the pain intensified, she was asking for morphine every half hour, and her WBC count crept up near 18k. Obviously, she needed an operation for definitive treatment but she'd been consistently refusing invasive procedures for the past several days. She had a terminal illness. Doing nothing was an understandable option. I spent a long time talking to the family, informing them and her of the options. You're in a bad way, I said. You're in no condition to tolerate another major abdominal operation, but dying from a bowel obstruction isn't pleasant either. I sat on the edge of her bed while her family crowded around, her husband in a chair holding her hand across from me. These moments in medicine are so raw and private and absolutely pure. As doctors, we are privileged to be able to participate in these intimate discussions of life and death. Almost like voyeurs, we walk into their lives when they are most vulnerable, when all pretense is washed away and the very essence of one's existence is at stake, and they welcome our presence, stranger that we are, because they need us there........She looked at her kids, then her husband. I can't do it anymore, she says. I just can't. I'm tired of it all. I want to rest. Can't you just give me something for the pain....
Her husband's head dropped and he squeezed her pale thin hand even tighter. Sure honey he said, his voicing barely holding together. We can do that. Right doctor? I nodded my head and rose slowly from the bed. Silently, I made my way out of the room; my privileged time had come to an end.
Monday, February 11, 2008
Zednik's Colombian Necktie
Harrowing case from the National Hockey League yesterday. Richard Zednik catches a teammates' skate blade in the neck and severs his carotid artery. Amazingly, he skates off the ice, leaving a trail of blood, and the trainers are able to get a pressure dressing on the wound. Based on the wire reports it sounds like a primary repair was done and the guy is doing pretty well.
Interestingly, outcomes after penetrating carotid injuries are much better than those seen after blunt carotid trauma. Blunt injuries tend to be associated with extensive dissections, mural thrombi, and higher incidences of stroke. A nice clean transection (like from a skate blade) will often temporarily go into spasm or clot off, allowing for re-approximation in the OR once the ends are cleaned up. The key thing is whether the patient presents with neurologic deficits and/or coma. Some advocate simply ligating the carotid if this is the scenario, as repair will not affect the outcome.
Interestingly, outcomes after penetrating carotid injuries are much better than those seen after blunt carotid trauma. Blunt injuries tend to be associated with extensive dissections, mural thrombi, and higher incidences of stroke. A nice clean transection (like from a skate blade) will often temporarily go into spasm or clot off, allowing for re-approximation in the OR once the ends are cleaned up. The key thing is whether the patient presents with neurologic deficits and/or coma. Some advocate simply ligating the carotid if this is the scenario, as repair will not affect the outcome.
Sunday, February 10, 2008
Journal Review

Cold, snowy day in Cleveland area. Great time to get caught up on some reading. I've been churning through some journals; here's some highlights.
From Journal of the American College of Surgeons:
1. The neverending debate of hypertonic saline vs LR/normal saline in trauma fluid resuscitation will be revisited with a multicenter, randomized controlled trial comparing 28 day survival for the hypotension cohort and 6-month neurologic outcomes in the traumatic brain injury cohort. Patients will be randomized to either an initial 250cc bolus of 7.5% hypertonic saline, 7.5% saline with dextran, or .9% normal saline. After this initial fluid infusion, resuscitation is to proceed via usual institutional protocol.
Problems: Patients can receive up to 2 liters of IV fluid prior to enrollment in the study. Seems to me that presence or absence of pre-enrollment resuscitation is a potential confounding factor. Also, once the 250 cc blous is given, the patient gets any additional fluid support deemed appropriate. This means that someone may get his 250 cc of hypertonic saline, only to be followed by 6 or 7 liters of regular crystalloid, or even blood. How do you know if "differences" are more a reflection of the particular treatment arm or of the adequacy of overall resuscitation?
2. A good article on the importance of adequate lymphadenectomy in colon resections for colorectal cancer of the elederly (78 years old). This was a retrospective review of the National Cancer Data Base from 1998-2004. Standard of care is to remove at least 12 lymph nodes in segmental resections for colon cancer. Less than 12 can lead to understaging and compromised survival. The study suggests that patients older than 78 are more likely to have inadequate lymphatic sampling. I can see how this might have arisen; sometimes when doing major abdominal surgery on a frail, elderly patient, surgeons will want to just "get the thing out" as quickly as possible. Short cuts are taken. Maybe the mesentery isn't taken as high as it should. Maybe you skip the total mesenteric excision of rectal cancer. The idea is to remove the tumor as expeditiously as possible, trying to avoid the dangers of "high ligation" of vascular pedicles. Certainly in any oncologic operation, proper technique is paramount. A relatively healthy elderly patient with few co-morbidities deserves a proper operation, just as someone in their forties. But sometimes you get called for a bleeding cancer on a 90 year old guy with COPD/CAD, multiple abdominal operations, and the family doesn't want him to die of exsanguination.... it's a judgment call and as we take care of more patients in their ninth and tenth decades, you have to be careful insisting on "standards of care" in all situations.
3. "Significance of Sentinel Lymph Node micrometastases in breast cancer". Great learning article. This was a single institution retrospective review of over 2000 patients with sentinel lypmph nodes showing micrometastatic or no micrometastatic disease.
First, some terminology:
N0(i-): node negative with both H&E and immunohistochemistry (IHC) staining
N0(i+): node negative with H&E, but microscopically positive (up to .2mm) on IHC
N1(mi): node positive with H&E (size between .2 and 2mm)
Surgeons will usually perform completion axillary dissections with H&E positive sentinel nodes. The controversy recently has been what to do about sentinel nodes microscopically positive in IHC staining. Theoretically, omission of axillary dissection in these patients can lead to understaging of disease.
In this study, additional positive, non sentinel, lymph nodes were identified in 15.5% of patients with N1mi sentinel pathology, and 9.3% of patients with N0(i+) sentinel pathology. Interestingly, although survival was no different in patients with N0(i-) vs N0(i+) sentinel nodes, decreased survival was seen in N0(i+) patients when completion axillary dissection was omitted. Although not a randomized controlled trial, this article seems to suggest that even micrometastatic disease can portend poorer outcomes if completion axillary dissection is not done. Until things are clarified, I'll continue to do the dissection in micrometastatic disease....
4. A good study from Sloan-Kettering on the utility of MRI in the always difficult to manage setting of Paget's Disease of the breast.
Well, I was going to go through Annals and Archives of Surgery but.... this actually takes a long time and the Cavs are on soon and it's Sunday night and we're in full-fledged blizzard mode and I think it might be time for a cocktail...hopefully I'll get to them later this week.
Thursday, February 7, 2008
One man's take
Everyone else is doing it; I figured it was time to articulate some sort of stance on the "health care crisis". It's an issue I've been vaguely aware of for a long time, but hadn't put any real thought into it because, truthfully, I was pretty ignorant of the issues and options. I've never been one to get involved in political issues. I wasn't the class president sort of guy. I'm a grinder. I like to show up evey day, take care of patients, operate, and let the "smart people" figure out what to do about compensation and coverage. But with the upcoming election, it has become apparent that universal health care has become a lightning rod issue. Change is on the horizon. The present system isn't working. We live in the wealthiest country in the history of the world and millions of people either have no coverage at all, or inadequate coverage. ER's have turned into overcrowded dumping grounds where people go when they're too sick to go anywhere else. This patchwork quilt of multiple private insurance plans casts too narrow of a net. Employment based insurance works well when everyone in town works at the steel mill or the auto plant, but that paradigm of employment is disintegrating in America.
No one spends more per capita on health care than the United States. So where is all that money going? Why are there have-nots amongst us?
You have to start with a Defining Principle. Ask yourself, is it a fundamental human right to have access to health care? Your answer to that will guide all subsequent decision making. By a "right" this means not only that one has access, but that the provision of such access does not cause one to tumble into financial ruin. Showing up in the ER with a severe headache and being sent home with tylenol after a negative CT scan will get you a bill for several thousand dollars. Does every American citizen have a "right" to adequate preventive and emergency healthcare, or is health care merely another "commodity" to be purchased or earned? That's the issue. It's as simple as that. Where do you stand? For comparison, consider housing or sustenance. Are these human rights? Do you have a right to eat? Is health care the same type of issue?
Universal health care can come in two conceivable flavors. One would be a single payor system, presumably government run, that would be available to every American citizen. We're talking cradle to grave, socialistic health care. Your kid comes down with strep throat? Take him to the pediatrician and don't worry about co-pays. You're having severe abdominal pain? Go to the ER and get your CT scan, US, whatever it takes. The other form of universal health care would involve some combination of government programs(Medicaid) and an expansion of private health insurance. This is where the concept of "mandates" come into play. Just like it's illegal to drive a car without insurance, you would be required, with government subsidization in the form of either tax rebates or lump sum payments, to purchase a basic minimum of health insurance from the private insurer of your choice. In this system, free enterprise and the open market system is preserved.
Several questions:
1. I spent a substantial part of my training years working at Cook County Hospital. This was a government subsidized charity hospital. And it was a shit hole. Patients waited 6 months to have giant, painful inguinal hernias hoisted out of their scrotums. Women waited weeks for their breast surgery. The place smelled and too many of the employess didn't give a damn. Physicians who have trained at VA's and county hospitals across the nation will concur; the government doesn't exactly have a good historical track record running the show in the health care business. How will they do when the entire country falls under their domain?
2. What will happen to Kaiser and all the HMO's if a single payor system were implemented? Do they go out of business? Is this illegal? Is it fair? We're talking about shutting down multi-billion dollar enterprises.
3. The mandate system is absurd. The sort of people without insurance are exactly the kind of people HMO's don't want in their plan. You don't think premiums are going to drift higher and higher? Are we looking at a future of $4000 deductibles?
4. Theoretically, medical expenditures have no definable cap. In fact, it's infinite. If enough money is available, it will get spent. Take for example the 89 year old demented guy who comes in with an UTI, develops a DVT, gets septic, half the hospital staff is consulted, he starts vomiting, CT scans are ordered, he crashes, is intubated, etc etc. You could describe his hospital course as a series of problems, each with a diagnostic confirmation and an appropriate treatment plan. Or you could say: an old guy came into the hospital and embarked on the dying process. Thereby skipping alot of the nonsense and expense. The deal is, at some point, if you want to make health care available for everyone, rationing is going to be an inevitable component of making it financially viable.
5. How do doctors get paid? Do we become employees of Uncle Sam? What happens to quality of care if physician salaries drop so far as to make medicine an unappealing career choice. (Glorified civil servants).
6. Will a two-tiered system develop? The top tier consisting of upper middle class and wealthy Americans who can afford so-called concierge care and get their procedures done quickly and conveniently at stand alone boutique surgicenters. I have a friend who maintains this isnt a horrible thing. If you're receiving foodstamps, you oughn't be able to buy filet mignon and a bottle of beaujolais. Hamburger and milk and eggs, no problem.
7. When are we going to explicitly define "futile care"? When are we going to make it mandatory for patients in hospitals to have DNR/End of Life forms completed upn admission?
Sometimes, it's just too mind boggling to think we will be able to efficiently reform our broken system in the foreseeable future. The uninsured are a drain on society, no doubt. But it goes deeper than that. The well-insured demented gork who sucks thousands of dollars every day out of the ICU is just as much a drain. We have CEO's of for-profit HMO's raking home 7 figure salaries; but what did you expect? That's what CEO's of private companies are supposed to make. So why are private companies in control of doling out our health care dollars? It makes my head spin. I have a case now.... let me know when somebody comes up with the panacea....
No one spends more per capita on health care than the United States. So where is all that money going? Why are there have-nots amongst us?
You have to start with a Defining Principle. Ask yourself, is it a fundamental human right to have access to health care? Your answer to that will guide all subsequent decision making. By a "right" this means not only that one has access, but that the provision of such access does not cause one to tumble into financial ruin. Showing up in the ER with a severe headache and being sent home with tylenol after a negative CT scan will get you a bill for several thousand dollars. Does every American citizen have a "right" to adequate preventive and emergency healthcare, or is health care merely another "commodity" to be purchased or earned? That's the issue. It's as simple as that. Where do you stand? For comparison, consider housing or sustenance. Are these human rights? Do you have a right to eat? Is health care the same type of issue?
Universal health care can come in two conceivable flavors. One would be a single payor system, presumably government run, that would be available to every American citizen. We're talking cradle to grave, socialistic health care. Your kid comes down with strep throat? Take him to the pediatrician and don't worry about co-pays. You're having severe abdominal pain? Go to the ER and get your CT scan, US, whatever it takes. The other form of universal health care would involve some combination of government programs(Medicaid) and an expansion of private health insurance. This is where the concept of "mandates" come into play. Just like it's illegal to drive a car without insurance, you would be required, with government subsidization in the form of either tax rebates or lump sum payments, to purchase a basic minimum of health insurance from the private insurer of your choice. In this system, free enterprise and the open market system is preserved.
Several questions:
1. I spent a substantial part of my training years working at Cook County Hospital. This was a government subsidized charity hospital. And it was a shit hole. Patients waited 6 months to have giant, painful inguinal hernias hoisted out of their scrotums. Women waited weeks for their breast surgery. The place smelled and too many of the employess didn't give a damn. Physicians who have trained at VA's and county hospitals across the nation will concur; the government doesn't exactly have a good historical track record running the show in the health care business. How will they do when the entire country falls under their domain?
2. What will happen to Kaiser and all the HMO's if a single payor system were implemented? Do they go out of business? Is this illegal? Is it fair? We're talking about shutting down multi-billion dollar enterprises.
3. The mandate system is absurd. The sort of people without insurance are exactly the kind of people HMO's don't want in their plan. You don't think premiums are going to drift higher and higher? Are we looking at a future of $4000 deductibles?
4. Theoretically, medical expenditures have no definable cap. In fact, it's infinite. If enough money is available, it will get spent. Take for example the 89 year old demented guy who comes in with an UTI, develops a DVT, gets septic, half the hospital staff is consulted, he starts vomiting, CT scans are ordered, he crashes, is intubated, etc etc. You could describe his hospital course as a series of problems, each with a diagnostic confirmation and an appropriate treatment plan. Or you could say: an old guy came into the hospital and embarked on the dying process. Thereby skipping alot of the nonsense and expense. The deal is, at some point, if you want to make health care available for everyone, rationing is going to be an inevitable component of making it financially viable.
5. How do doctors get paid? Do we become employees of Uncle Sam? What happens to quality of care if physician salaries drop so far as to make medicine an unappealing career choice. (Glorified civil servants).
6. Will a two-tiered system develop? The top tier consisting of upper middle class and wealthy Americans who can afford so-called concierge care and get their procedures done quickly and conveniently at stand alone boutique surgicenters. I have a friend who maintains this isnt a horrible thing. If you're receiving foodstamps, you oughn't be able to buy filet mignon and a bottle of beaujolais. Hamburger and milk and eggs, no problem.
7. When are we going to explicitly define "futile care"? When are we going to make it mandatory for patients in hospitals to have DNR/End of Life forms completed upn admission?
Sometimes, it's just too mind boggling to think we will be able to efficiently reform our broken system in the foreseeable future. The uninsured are a drain on society, no doubt. But it goes deeper than that. The well-insured demented gork who sucks thousands of dollars every day out of the ICU is just as much a drain. We have CEO's of for-profit HMO's raking home 7 figure salaries; but what did you expect? That's what CEO's of private companies are supposed to make. So why are private companies in control of doling out our health care dollars? It makes my head spin. I have a case now.... let me know when somebody comes up with the panacea....
Monday, February 4, 2008
cecal volvulus

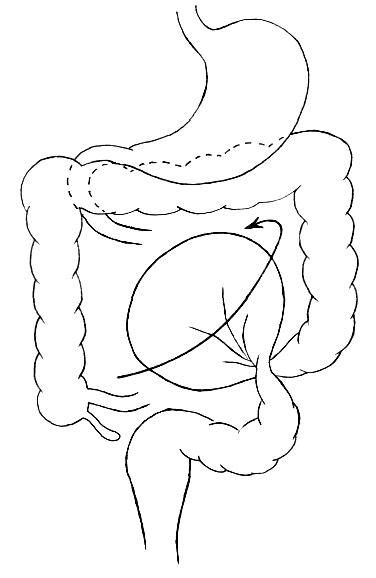
56 year old lady with acute onset of severe abdominal pain and nausea. She had a hysterectomy 20 years ago, no other operations. Overall, a pretty healthy lady. This was one of those calls you get in the middle of the night with a vague preliminary CT read: Small bowel obstruction, cannot rule out a million other things. Her labs were ok so I had them place an NG and admit her. When I examined her early this morning, I was a little concerned. She had focal peritoneal signs in the RLQ and also in the epigastrium. She was also distended with tympany, but the distention interestingly enough, was asymmetric; right sided predominance. The radiologist who reviews the Nighthawk scans from the night before called me and expressed concern about possible cecal volvulus. We went through the scan together and it seemed compelling to me. I re-examined her and recommened at least sticking a scope in. As soon as I established pneumoperitoneum and slipped in the laparoscope, I started telling the team to open up the laparotomy packs. Her cecum was the size of a basketball, flopped over medially and pointing toward the LUQ. Cecal volvulus. I opened her up, detorsed the entire ascending colon and performed a standard right hemicolectomy. There were some patchy areas of ischemia but no frank gangrene.
Colonic volvulus is a cool disease process for a surgeon. It takes a little bit of thinking and work to diagnose and the treatment usually involves some sort of colectomy. It's a mechanical problem and definitve surgery is usually curative. It's pretty satisfying when all goes well.
"Volvulus" means twisting of the bowels, usually around it's mesenteric axis. Obstruction and ischemia are the most feared complications. Most cases of volvulus in the United States affect the sigmoid colon. What happens is you get a redundant loop of sigmoid on a narrow mesentery that can twist on itself. We usually see this in older, debilitated, institutionalized patients. Chronic constipation plays a role. Initially you try to decompress the volvulus with either a flex sigmoidoscope or barium enema. The you can electively do a one stage colectomy after a bowel prep.
{kind=link}
Cecal volvulus is a little bit of a misnomer. It isn't just the cecum that volvulizes. The entire ascending colon lacks normal fixation to the retroperitoneum and you get cecocolonic twisting around the ileocolic vascular pedicle. Patients will present with apparent distal small bowel obstruction and decompressed distal transverse colon. Contrary to sigmoid volvulus, non-operative decompressive techniques for cecal volvulus are unsatisfactory. You have to take these patients to the OR. I did a right hemicolectomy because I think that is the safest, most definitve operation. People have described simply performing a cecopexy and placing cecostomy tubes, but I think those options are fraught with complications and carry unacceptably high recurrence rates. Certainly, if the patient is toxic and unstable, with advanced bowel ischemia, you might have to consider a temporary ileostomy with mucous fistula.
Sunday, February 3, 2008
Super Sunday
I got tired of blogging for a while. It happens. But then you check your site and you see the same damn post day after day, and that gets even more annoying and depressing. So it's halftime of the Super Bowl and I'm watching a disturbingly older-looking and bizarre Tom Petty "rocking out" and I think maybe I'll write something instead. So here's some random unconnected thoughts.
1. Three spleens in a 10 day period. Never thought it possible outside a major level I trauma center. I know I had a previous post where there was gnashing of teeth regarding whether I did the right thing, but by the third one, there was no hesitation. Peritonitis? Check. Hemodynamic tenuousness? Check. Awful-looking CT scan? Check. Out with your spleen, young man.
2. There's an entity in suburban general surgery known as the "vacation home gallbladder". These are the referrals for lap chole on patients who maybe don't really need surgery. The "complicated" (aka crazy) 47 year old single woman with chronic abdominal pain who has been admitted to the hospital seven times in the last six months, multimillion dollar workups, scoped up and down, no diagnosis, maybe it's the gallbladder, refer to the surgeon sort of case. You take those gallbladders out and bank the reimbursement in the vacation home fund. I got called last week on a 88 year old lady, pleasantly demented, who was admitted with mental status changes and dehydration. Basically she had a UTI. Workup, though, demonstrated mildly elevated AST/ALT (liver function tests). For some reason US and HIDA scans were ordered. The gallbladder filled on the HIDA normally, but with cholecystokinin her ejection fraction was only 8%. Less than 30% is considered abnormal. But this lady was asymptomatic. She had no pain. I saw her and she was sitting up in a chair with the TV on some televangelist and there were corn flakes stuck to her chin. She smiled and told me good morning. I pushed her belly a little bit and she kept smiling. I respectfully declined to book her for lap chole. There's better ways of making buck. General surgeons who do these cases, rest assured, are trying to make that second mortgage payment on a condo on Kiawah Island.
3. Al Qaeda apparently has run out of young impressionable men to brainwash for their suicide missions. Who do you turn to when you want someone to blow themselves up in a crowded shopping center? Well, the mentally retarded of course. I don't think I've heard a more reprehensible, more morally bankrupt story in my life. It's just sick.
4. 3:10 to Yuma an excellent flick.... rent it.
5. New absorbable tack on the market for ventral lap hernias.... going to try it next week.
6. Brady looks rattled. Giants got a shot.
1. Three spleens in a 10 day period. Never thought it possible outside a major level I trauma center. I know I had a previous post where there was gnashing of teeth regarding whether I did the right thing, but by the third one, there was no hesitation. Peritonitis? Check. Hemodynamic tenuousness? Check. Awful-looking CT scan? Check. Out with your spleen, young man.
2. There's an entity in suburban general surgery known as the "vacation home gallbladder". These are the referrals for lap chole on patients who maybe don't really need surgery. The "complicated" (aka crazy) 47 year old single woman with chronic abdominal pain who has been admitted to the hospital seven times in the last six months, multimillion dollar workups, scoped up and down, no diagnosis, maybe it's the gallbladder, refer to the surgeon sort of case. You take those gallbladders out and bank the reimbursement in the vacation home fund. I got called last week on a 88 year old lady, pleasantly demented, who was admitted with mental status changes and dehydration. Basically she had a UTI. Workup, though, demonstrated mildly elevated AST/ALT (liver function tests). For some reason US and HIDA scans were ordered. The gallbladder filled on the HIDA normally, but with cholecystokinin her ejection fraction was only 8%. Less than 30% is considered abnormal. But this lady was asymptomatic. She had no pain. I saw her and she was sitting up in a chair with the TV on some televangelist and there were corn flakes stuck to her chin. She smiled and told me good morning. I pushed her belly a little bit and she kept smiling. I respectfully declined to book her for lap chole. There's better ways of making buck. General surgeons who do these cases, rest assured, are trying to make that second mortgage payment on a condo on Kiawah Island.
3. Al Qaeda apparently has run out of young impressionable men to brainwash for their suicide missions. Who do you turn to when you want someone to blow themselves up in a crowded shopping center? Well, the mentally retarded of course. I don't think I've heard a more reprehensible, more morally bankrupt story in my life. It's just sick.
4. 3:10 to Yuma an excellent flick.... rent it.
5. New absorbable tack on the market for ventral lap hernias.... going to try it next week.
6. Brady looks rattled. Giants got a shot.
Subscribe to:
Posts (Atom)