
56 year old lady with acute onset of severe abdominal pain and nausea. She had a hysterectomy 20 years ago, no other operations. Overall, a pretty healthy lady. This was one of those calls you get in the middle of the night with a vague preliminary CT read: Small bowel obstruction, cannot rule out a million other things. Her labs were ok so I had them place an NG and admit her. When I examined her early this morning, I was a little concerned. She had focal peritoneal signs in the RLQ and also in the epigastrium. She was also distended with tympany, but the distention interestingly enough, was asymmetric; right sided predominance. The radiologist who reviews the Nighthawk scans from the night before called me and expressed concern about possible cecal volvulus. We went through the scan together and it seemed compelling to me. I re-examined her and recommened at least sticking a scope in. As soon as I established pneumoperitoneum and slipped in the laparoscope, I started telling the team to open up the laparotomy packs. Her cecum was the size of a basketball, flopped over medially and pointing toward the LUQ. Cecal volvulus. I opened her up, detorsed the entire ascending colon and performed a standard right hemicolectomy. There were some patchy areas of ischemia but no frank gangrene.
Colonic volvulus is a cool disease process for a surgeon. It takes a little bit of thinking and work to diagnose and the treatment usually involves some sort of colectomy. It's a mechanical problem and definitve surgery is usually curative. It's pretty satisfying when all goes well.
"Volvulus" means twisting of the bowels, usually around it's mesenteric axis. Obstruction and ischemia are the most feared complications. Most cases of volvulus in the United States affect the sigmoid colon. What happens is you get a redundant loop of sigmoid on a narrow mesentery that can twist on itself. We usually see this in older, debilitated, institutionalized patients. Chronic constipation plays a role. Initially you try to decompress the volvulus with either a flex sigmoidoscope or barium enema. The you can electively do a one stage colectomy after a bowel prep.
{kind=link}
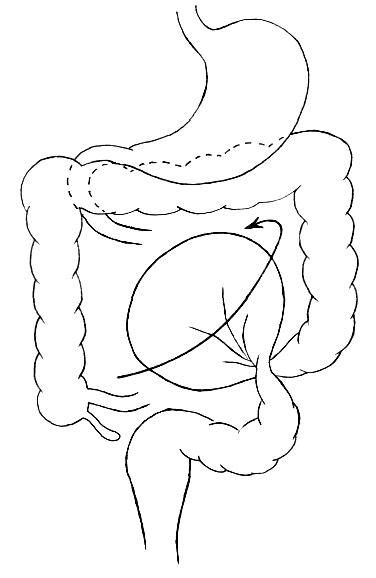
Cecal volvulus is a little bit of a misnomer. It isn't just the cecum that volvulizes. The entire ascending colon lacks normal fixation to the retroperitoneum and you get cecocolonic twisting around the ileocolic vascular pedicle. Patients will present with apparent distal small bowel obstruction and decompressed distal transverse colon. Contrary to sigmoid volvulus, non-operative decompressive techniques for cecal volvulus are unsatisfactory. You have to take these patients to the OR. I did a right hemicolectomy because I think that is the safest, most definitve operation. People have described simply performing a cecopexy and placing cecostomy tubes, but I think those options are fraught with complications and carry unacceptably high recurrence rates. Certainly, if the patient is toxic and unstable, with advanced bowel ischemia, you might have to consider a temporary ileostomy with mucous fistula.
17 comments:
Is that the actual AXR?
Impressive photo! and nice post.
The one and only Sid Schwab will be visiting The Doctor Anonymous Show on February 7th, 2008 at 9pm eastern time. I invite you and your readers to take part in this unique opportunity to interact with this well known medblogger. Check out my blog for details.
i love your x-rays and ct scans.
just for interest sake, sigmoid volvulus is pretty common in my neck of the woods, but not the western type. i posted on it some time ago. take a look at
http://other-things-amanzi.blogspot.com/2007/07/tough-surgeon.html
Boy, if that's the actual XRay, someone blew it. (Not you -- I mean the person who called you with a "SBO."
One of my worst cases ever, very early in my practice, was a woman with cecal volvulus whose xray did not show it. I operated about 12 hours after I saw her, which was two days after her original hospitalization at another hospital. Her cecum was torsed but most likely viable, but I took it out anyway. After a very smooth operation and what should have been a normal recovery, she began an unrelenting downward slide, due to suppurative pyelephlebitis. I suppose the seeds were sewn even before I saw her; but detorsing always gives me the creeps now, and I've often applied a clamp to the twisted mesentery before I do it, wondering if seeding during that maneuver had anything to do with the patient's demise...
Not the actual xray... our hospital switched to some new digital radiology system that requires me to call and order a copy of the CD.... pain in my ass.....but it is a cool pic.
Doc Schwab- I read that post about the pyelephlebitis... horrible luck; doubt the detorsing led to her downward spiral.
I've actually heard a couple senior surgeons at my hospital talk about the "evil humors" that are release systemically when the bowel is detorsed -> ARDS, MODS, etc. These guys recommend, as Dr. Schwab mentioned, clamping the mesentary as well before manipulating the bowel if possible.
hi dr. jeffrey, could please describe the caecal volvulus x-ray?coz i'm not so good in reading AXR..looks to me that there's distended small bowel..but i don't knw whether u can see twisting caecum in tht AXR?thnx so much..
hi dr. jeffrey, could please describe the caecal volvulus x-ray?coz i'm not so good in reading AXR..looks to me that there's distended small bowel..but i don't knw whether u can see twisting caecum in tht AXR?thnx so much..
Salmora- That giant air blob you see in the middle of the abdomen is the cecum.
ooo..ic..the caecal volvulus is literally basketball size..i thought the gas in the middle of the abdomen is dilated small bowel..not solely caecal volvulus..thats really huge..
thnk u dr jeffrey for the description:)
Dr. Parks,
I totally thought I was reading a post by my doctor regarding my surgery on March 11th. I had pain in my right lower side, woke up at 11:00 PM with nausea, began projectile vomiting at 2:00 AM. Went to the ER and they discoverd that I had a cecal volvulus. I heard the Radiologist ask her tech, "Is that her whole cecum?" My doc said that my cecum was the size of my entire abdomen. What could cause that? I, too, was 56 and have had ashesions, however, my doc said that he didn't see many adhesions.
I did have previous surgery for bowel obstruction in 2001. I had two blockages...one in the lower right small intestine near my groin and one around the colon to the right of my navel. My doctor (different from my recent surgery) said that something (not adhesion's) had wrapped around my intestines and colon like the tentacles of an octopus. He, my doc, was 75 years old and said he had never seen anything like it. When I went to the hospital I knew I was blocked and thought it was due to adhesions, so I was surprised to hear that I had a volvulus. Since my surgery in March, I've done pretty well, but lately I've been having pain in my upper right bowel area. It's a burning, tearing kind of pain. Do you have any idea what could be causing that? My doctor wasn't that great and he discharged me 2 weeks after my surgery. Do I call him or see someone else?
Thanks for any info you might have. I try to take care of myself, take no meds and am relatively healthy.
Sincerely,
S. Forbes
Dr. Schwab,
Great posting!!!
Do you take referrals?
I have been trying to let the doctors know for over 2 years after my Hysterectomy that there was something wrong on the inside of my right groin. I have recently had a CT enteroclysis and the findings left me with a notable cecum occupies a low position in the right hemipelvis and a redundant transverse colon dips inferiorly with the mid portion of the transverse colon also in the low mid pelvis. (absent Uterus).
I'll call your office tomorrow. Perhaps you can assist my current physicians with helping me get the right solution.
I have some concerns that when the hernia surgeon sutured my nerve to the pubic bone it left me with lack of blood flow throughhout the right side of my lower body to my feet. I was left with nerve damage also. I have most of the symptoms of the Mesenteric Ischemia. I can only eat in small amounts due to the pain that radiates from the cecum area (usually detends) to the labia and vulva.
signed: Help Please
Dear Dr. Buckeye Surgeon,
Sorry I used the wrong name.
Great posting!!!
Do you take referrals?
I have been trying to let the doctors know for over 2 years after my Hysterectomy that there was something wrong on the inside of my right groin. I have recently had a CT enteroclysis and the findings left me with a notable cecum occupies a low position in the right hemipelvis and a redundant transverse colon dips inferiorly with the mid portion of the transverse colon also in the low mid pelvis. (absent Uterus).
I'll call your office tomorrow. Perhaps you can assist my current physicians with helping me get the right solution.
I have some concerns that when the hernia surgeon sutured my nerve to the pubic bone it left me with lack of blood flow throughhout the right side of my lower body to my feet. I was left with nerve damage also. I have most of the symptoms of the Mesenteric Ischemia. I can only eat in small amounts due to the pain that radiates from the cecum area (usually detends) to the labia and vulva.
signed: Help Please
April 6, 2009 5:12 PM
I am dealing with a caecal volvulus.
Acute onset abdominal pain . X.ray show small bowel dilatation.
Laparoscopy confirmed caecal volvulus. Untwisted it and fixed to lateral wall with three stitches.
Patient very well . X.ray show caecum in normal position and air in teh transverse colon.
I had mere detorsion in 1998 and right hemicolectomy in 2000. Quite a ride. The other day had symptoms that resembled the early stages of the acute episodes--complete freakout.
I had a recent CT that said I have a cecal bascule. I've been told I don't need to be concerned about it. I'm not symptomatic. Should I really ignore it?
Post a Comment