There are few emergencies in biliary disease. Run of the mill biliary colic can be managed as an outpatient. Even patients with acute cholecystitis can be cooled down for 24-48 hours with fluids and IV antibiotics prior to definitive surgery. But a patient presenting with ascending cholangitis is another matter. Delays in intervention can be life threatening.
The fundamental problem with cholangitis is some obstruction of the common bile duct. Most commonly, the cause is from a gallstone that trickles out of the gallbladder and lodges itself in the distal duct. Other etiologies include strictures and tumors. The bile flow is stanched and the patient will become jaundiced. Pooled bile is a terrific medium for bacterial overgrowth and gram negative organisms such as e. coli and klebsiella can superinfect the biliary system. The end result is purulent bile under pressure and, with the common duct obstructed, it decompresses back into the liver, accessing the systemic bloodstream via the portal triads. Bacteremia and rampant sepsis ensues.
I saw a patient the other week who had been admitted through the ER with a diagnosis of "sepsis". When I walked into the room she was in extremis. She was frankly jaundiced and had one of those wide-eyed looks of horror on her face. Her systolic blood pressure was in the seventies and she was breathing 40 times a minute. Her thighs were mottled bluish-black in a marbled pattern and her fingers and toes were dusky and cold. She was maxed out on levophed and vasopressin. Her white count was 20k and her bilirubin was over 10. On exam she could only mumble incoherently on questioning. Her abdomen was distended and she had diffuse peritoneal signs. We rapidly obtained control of her airway and pondered the next move.
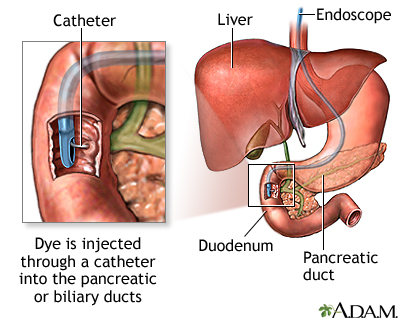
For most patients with ascending cholangitis, the best initial move is an ERCP (endoscopic retrograde cholangiopancreatography). ERCP is both diagnostic and therapeutic. A sphincterotomy can be done to open up the ampulla and stones impacted in the distal duct can be scooped out with a basket retriever. Relief is often immediate. Much like a boil that feels better after it's lanced, ERCP will usually lead to rapid improvement in the patient's condition. Subsequently, the patient can then undergo a laparoscopic cholecystectomy to remove the source of the problem.
{kind=link}
This patient was a different situation. Not too many GI interventionalists are going to be too excited about doing an ERCP on an unstable patient. Although we could have placed a PTC drain (percutaneous transhepatic cholangiography)for immediate decompression, I was concerned about her diffuse peritoneal signs. I wanted to have a look inside myself. Sometimes the safest course of action in these situations is to get a very ill patient on an OR table with some general anesthesia. Upon entering the peritoneal cavity I encountered bilious ascites and the gallbladder was frankly gangrenous. After washing everything out and doing a quick cholecystectomy, I performed a Kocher maneuver (mobilization of the duodenum)and I could palpate several hard stones in the distal common bile duct. A choledochotomy was made and I used a Fogarty balloon catheter to extract several stones. A cholangiogram conformed clearance of the duct and I closed the choledochotomy around a T-tube. Anesthesia was able to get her almost completely off the levophed by the time I was done.
{kind=link}
{kind=link}
This was a very unusual case. We seen patients jaundiced with common duct stones quite frequently in surgical practice but it's quite rare for a patient to progress so quickly to septic shock. Charcot's Triad (RUQ pain, fever, jaundice) is the classic descriptor of ascending cholangitis. It's the question every medical student rotating through a surgical service gets asked. Lesser known, and more ominous, is Reynaud's Pentad. In addition to pain/fever/ jaundice, hypotension and mental status changes are seen in this more severe variety of ascending cholangitis. This was the first time I've seen manifestations of Reynaud's Pentad in an actual patient.....
10 comments:
Interesting story.
Why is one of the first things you do obtaining an airway? Do you expect the airway to become obstructed at some point?
The t-tube picture you link to is blocked by firefox/google because of malicious content on that website...
Not something you want to see often. Impressive when you do.
as always, you d'man!!
was this really the first time she presented with ruq pain and stones? surprised she got to this point with her gallbladder not in a pan before then. great blog, by the way.
Anon 11:56-
You can't do anything with a dead patient. The patient was tachypneic to the 40s and had been so for an undetermined period of time. At some point anyone breathing that fast will tire suffer respiratory collapse. It is prudent to secure an airway in any such patient.
assuming you can't reliably return the patient to normal respiratory function relatively rapidly (ie an asthmatic who is in the 40s which you can (maybe) rapidly reverse medically).
Fascinating case. In 3 years of residency, I haven't seen Reynold's pentad either. The board answer for this pt would be biliary compression though, right? Unless you had a clinical reason to suspect gangrenous cholecystitis. I assume your US or CT showed the gall bladder nastiness. If you had no imaging, would you have still lapped her?
with regard to the previous comment, I meant "biliary decompression" not "biliary compression"
Anon-
Yes, ERCP is the ideal first maneuver. I wouldn't trust PTC or a cholecystostomy tube in a patient this sick. At that point it's a surgical emergency and you don't have a choice....
Post a Comment